
This 23-year-old man had an out-of-hospital cardiac arrest one hour after playing hockey. He was successfully resuscitated.
This ECG was recorded 2 weeks later, when he was transferred to a tertiary care cardiac center:
- Sinus bradycardia, 58/min, with interpolated premature ventricular complexes (“interpolated” PVCs are sandwiched between two consecutive regular complexes and are not followed by a pause)
- Prolonged QT (QT = 666 msec, QTc = 659 msec)
The patient had been previously healthy and exercised frequently and vigorously. He had no history of palpitations, dizziness or syncope. One paternal uncle died suddenly at age 32, while eating breakfast one day before his wedding. His mother’s father diied suddenly at age 60.
A thorough non-invasive investigation was carried out after the episode of cardiac arrest . The marked QT prolongation was the only abnormality. Genetic tests to find the mutation causing the long-QT syndrome were positive for long QT syndrome type 2 (LQTS2).
During the 2 weeks following the cardiac arrest the patient had been on adequate doses of a beta-blocker and had recurrent episodes of self-terminating polymorphic ventricular tachycardia (PVT). Implantation of an AICD dual-chamber Automated Implantable Cardioverter-Defibrillator) was therefore planned.
This ECG was recorded 9 hours after the first. The patient had not experienced recurrence of polymorphic ventricular tachycardia during the interval: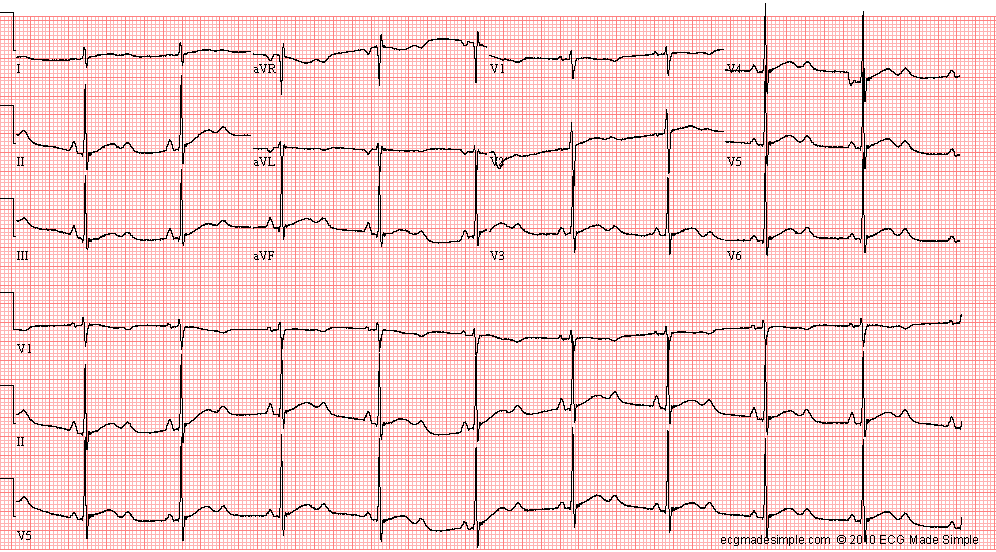
- Sinus rhythm, 58/min
- Right atrial enlargement
- Prolonged QT ( QT/QTc = 574/583 msec)
The ECG of patients with LQT2 mutation characteristically shows notched “bifid” T waves, with a late peak “T-U pattern”. The first ECG had a “giant T-U” that has been noted to occur in long QT syndrome patients at imminent risk of tordades de points.
For further information surrounding Long QT Syndrome, we recommend reading the following article.