
This 71-year-old man endorses a six month history of episodic weakness and pre-syncope. In the past month, he reports losing consciousness on several occasions, with episodes lasting 10-30 seconds. He presents to the ED because of three episodes of syncope in the past 12 hours:
- Sinus rhythm, 68/mi
- First degree AV block (PR = 260 msec)
- Right bundle branch block
- Left anterior fascicular block
- Consider trifascicular block
When the ECG shows right bundle branch block, fascicular block and first degree AV block, “trifascicular block“ may be suspected (complete bifascicular block + incomplete block of the third fascicle). In reality, this pattern is often due to bifascicular block plus conduction delay at the level of the AV node or the common His bundle, rather than a true trifascicular block. A definitive diagnosis of trifascicular block would require His bundle recording.
An AHA/ACCF/HRS Scientific Statement on the Standardization and Interpretation of the Electrocardiogram in 2009 recommended to avoid the use of the term trifascicular block “because of the great variation in anatomy and pathology producing such a pattern”. However, the term is still widely used and is often a cause of confusion
The patient was admitted to the cardiac ward and monitored on telemetry. He had a repeat episode of syncope:
- Sinus rhythm
- Advanced AV block (high grade AV block) with 15 seconds of ventricular asystole
The following ECG is recorded a few minutes after the episode: 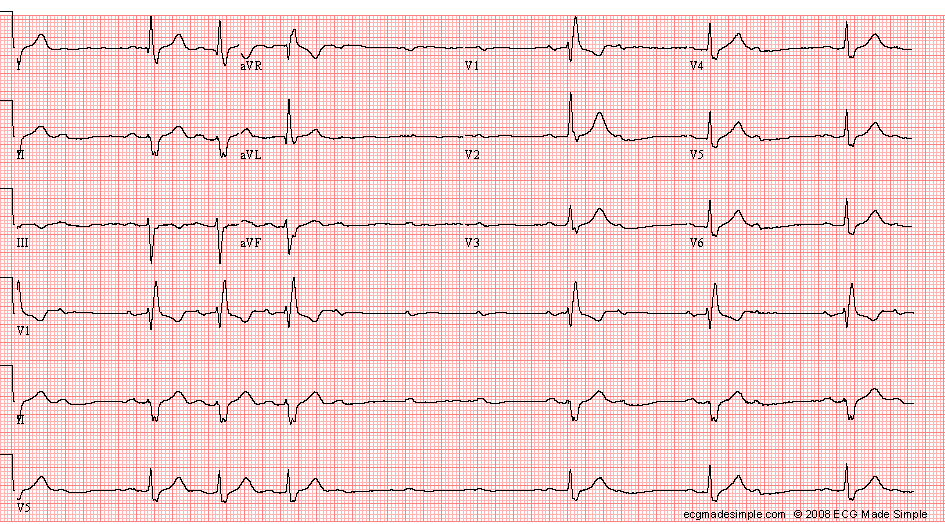
- Sinus rhythm with high grade AV block: Mobitz II second degree AV block and three successive non-conducted P waves
- Right bundle branch block
- Left anterior fascicular block
- Minimal criteria for left ventricular hypertrophy
The episode of asystole and the Mobitz II second degree AV block support the diagnosis of trifascicular block.
A VVI pacemaker is implanted: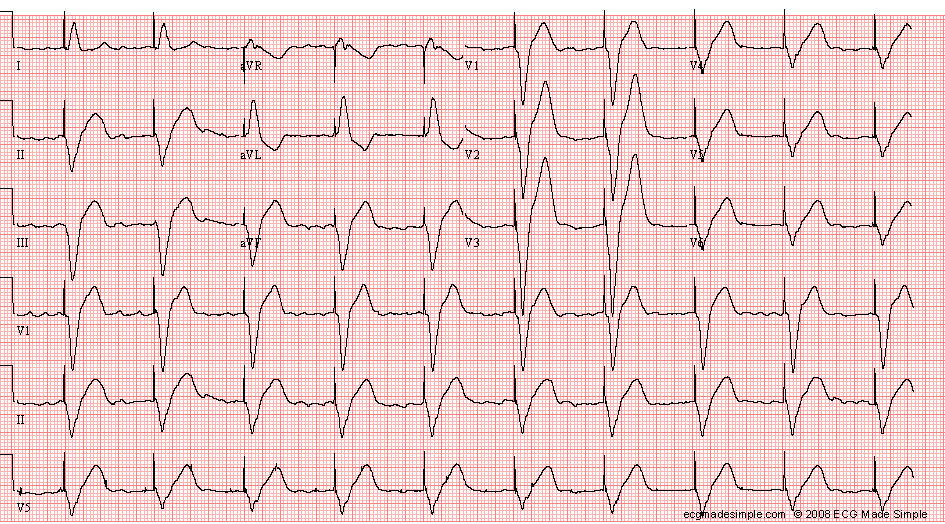
- Electronic ventricular pacemaker
- Atrial fibrillation
- Paced ventricular rhythm, 60/min
