
This 58-year-old man is being assessed by the anesthesia staff prior to prostatic surgery. He has no cardiac complaints. A routine ECG is obtained:

- In lead III the QRS complex is tiny (“collapsed”) and the P wave “invisible”
- The PQRST pattern in leads I and II is virtually identical and unusual
- The precordial leads are normal
- The ventricular rate is 60/min
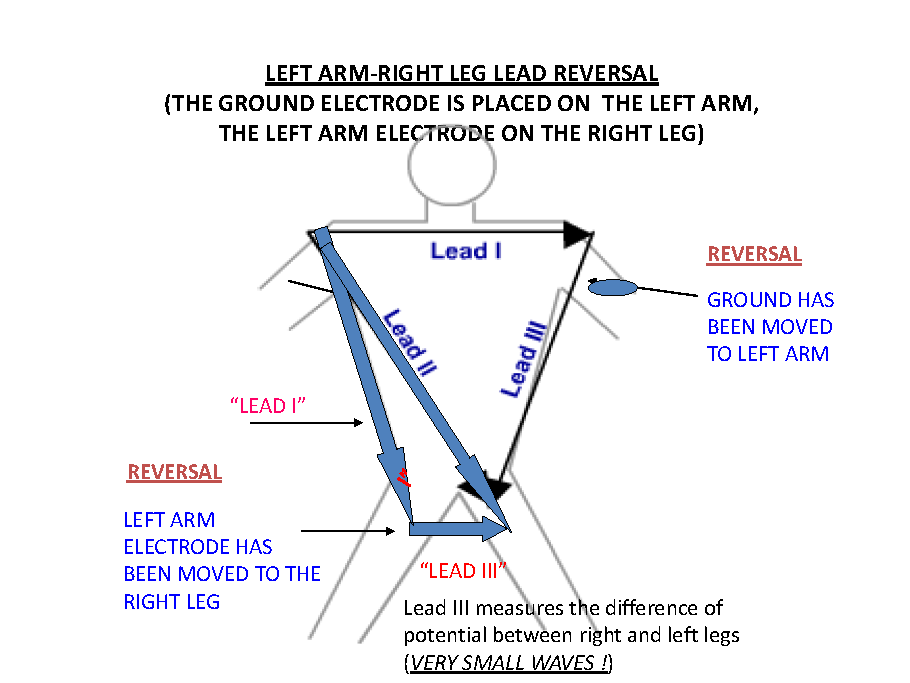
- Consider lead placement error (lead III is very likely measuring the potential difference between the legs….)

As a recording error is suspected, a second ECG is obtained, with particular attention to correct lead placement:

- Sinus rhythm, 60/min
- Minimal voltage criteria for left ventricular hypertrophy (R in aVL = 11 mm). It may be a normal variant
- A borderline ECG
Comment: The abnormalities in the previous tracings were due to a lead placement error A flat (“collapsed”) lead III is usually due to left arm-right leg lead reversal – Lead II, however should should not be affected by the placement error. See NEXT: Explanation
In Left Arm – Right leg reversal lead II should not be affected and should remain unchanged! (see diagram) We need an explanation!
There was indeed a double lead placement error: 1) right arm – left arm reversal 2) right arm – right leg reversal
In right arm – left arm reversal lead II is actually lead III and lead III is lead II. Therefore in the incorrectly recorded tracing the “collapsed lead” is actually lead II
