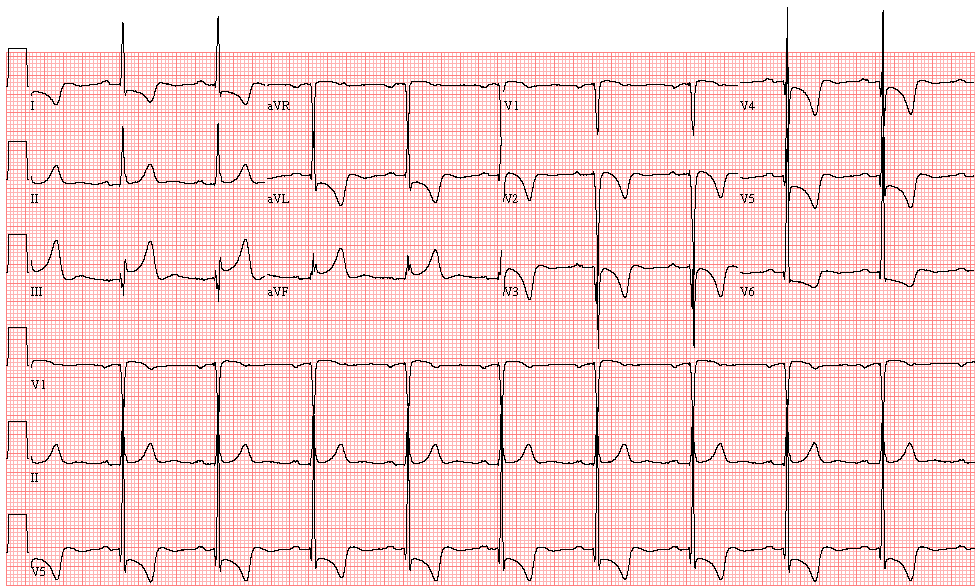
This 58-year-old man with a 10-year history of poorly treated hypertension is brought to the Emergency Department with severe lower retrosternal/epigastric pain for the past hour, as well as weakness and dyspnea:
- Sinus rhythm, 72/min
- Left ventricular hypertrophy with repolarization abnormality
- Septal myocardial infarction, age undetermined
- ST elevation in the inferior leads, consider acute inferior infarction
There was a significant elevation of serum cardiac troponins, in keeping with an acute myocardial infarction. Coronary angiography was carried out, which demonstrated total occlusion of the proximal segment of the left anterior descending artery. A thrombus was removed, and a stent was inserted, with good restoration of blood flow. The right and circumflex coronary arteries had only mild lesions.
The conclusion of the attending cardiologists was that the ST elevation in the inferior leads was reciprocal to the ST depression in leads I and aVL due to the left ventricular hypertrophy. The ST elevation remained unchanged during the following 10 days (see ECG 2 on the day of his discharge)
Following coronary angioplasty and stenting the patient is symptom-free. This ECG is recorded on the day of his discharge:
- Sinus rhythm, 69/min
- Left ventricular hypertrophy with repolarization abnormality
- Septal infarction
- ST elevation in the inferior leads (reciprocal to the ST depression in I and aVL due to LVH)
The patient was given a copy of his discharge ECG and advised to carry it, particularly when traveling, to prevent possible misdiagnosis of acute inferior infarction.
Eight months later, the patient was again brought to the Emergency Department with severe epigastric pain that he felt was similar to the discomfort he felt during his previous myocardial infarction. As he had been advised, he brought copies of his previous ECGs and a clinical note.
His electrocardiogram was unchanged, showing the marked ST elevation in the inferior leads. The serum cardiac troponins were normal. Further investigations demonstrated the presence of a peptic ulcer with moderate bleeding.
This case presents a good example of the importance of the patient carrying copies of ECGs and/or clinical information when there is a possibility of misdiagnosis.